Anatomy: Abdomen V - Stomach
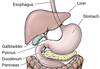
These flashcards detail the anatomy, capacity, and function of the stomach, the expanded section of the alimentary tract between the esophagus and small intestine. They highlight the stomach’s J-shape, variable position due to body type and physiological factors, and its role in digestion—converting food into chyme for transfer to the duodenum. The main anatomical parts (cardia, fundus, body, pyloric part) are also introduced, along with developmental and functional characteristics.
stomach
expanded part of the alimentary tract between the esophagus + small intestine
Key Terms
stomach
expanded part of the alimentary tract between the esophagus + small intestine
In most people, the shape of the stomach resembles___________?
What causes variations in the position of the stomach from person to person?
What causes variations in the position of the stomach in an individual?
normally = the letter J
person to person = body type<...
An empty stomach is only slightly larger than the large intestine;
How much food can it hold when expanded?
How much can a newborn’s stomach hold?
2 - 3 L of food
newborn = up to 30 mL of milk
What are the functions & specializations of the stomach?
specialized for:
accumulation of ingested food
The gastric juice gradually converts a mass of food into what?
Where is it passed to?
chyme - a semiliquid mixture
(passes quickly into duodenum)
What are the 4 parts of the stomach?
cardiafundus
body
Related Flashcard Decks
Study Tips
- Press F to enter focus mode for distraction-free studying
- Review cards regularly to improve retention
- Try to recall the answer before flipping the card
- Share this deck with friends to study together
| Term | Definition |
|---|---|
stomach | expanded part of the alimentary tract between the esophagus + small intestine |
In most people, the shape of the stomach resembles___________? What causes variations in the position of the stomach from person to person? What causes variations in the position of the stomach in an individual? | normally = the letter J person to person = body type individual variation:
|
An empty stomach is only slightly larger than the large intestine; How much food can it hold when expanded? How much can a newborn’s stomach hold? | 2 - 3 L of food newborn = up to 30 mL of milk |
What are the functions & specializations of the stomach? | specialized for:
functions:
(food blender and reservoir) |
The gastric juice gradually converts a mass of food into what? Where is it passed to? | chyme - a semiliquid mixture (passes quickly into duodenum) |
What are the 4 parts of the stomach? |
|
cardia | the part of the stomach surrounding the cardial orifice |
fundus |
|
The superior part of the fundus usually reaches what level? | left 5th intercostal space |
What is located between the esophagus and the fundus? | cardial notch |
The fundus may be dilated by …? | gas fluid food combination of these |
body of stomach | major part of the stomach between the fundus and the pyloric antrum |
pyloric part |
- pyloric antrum= wide part; leads into pyloric canal = narrow part |
The pylorus (distal, sphincteric region of the pyloric part) is a marked thickening of the circular layer of smooth muscle. | discharge of the stomach contents through the pyloric orifice into the duodenum |
When does intermittent emptying of the stomach occur? | when intragastric pressure overcomes the resistance of the pylorus |
What is the normal state of the stomach? What is an exception to this? |
except when emitting chyme |
What process passes the chyme through the pyloric canal + orifice into the small intestine for further mixing, digestion, and absorption? When does this occur? | gastric peristalsis
|
What are the 2 curvatures of the stomach? |
greater curvature |
Lesser curvature | forms the shorter concave border of the stomach |
Greater curvature | forms the longer convex border of the stomach |
angular incisure (notch) |
|
In a live patient, the interior of the stomach is covered by …? What protection does this provide? |
|
gastric folds (or gastric rugae) |
- folds diminish and obliterate as the stomach is distended (fills) |
A gastric canal (furrow) forms temporarily during swallowing between what structures? How can it be observed? |
|
Why does the gastric canal form? What passes through this canal? |
(no oblique layer at this site)
(to the pyloric canal when the stomach is mostly empty) |
What is the stomach covered by? What area is the exception to this? | peritoneum
|
The two layers of the lesser omentum extend around the stomach and leave its greater curvature as…? | as the greater omentum |
Anteriorly, the stomach is related to what 3 structures? | diaphragm left lobe of liver anterior abdominal wall |
Posteriorly, the stomach is related to what 2 structures? The posterior surface of the stomach forms most of the …? |
- anterior wall of the omental bursa |
From superior to inferior, the stomach bed is formed by what 6 structures? | left dome of diaphragm spleen left kidney + suprarenal gland, splenic artery pancreas transverse mesocolon + colon |
Pancreatic pseudo-cysts and abscesses in the omental bursa may do what to the stomach? How can physicians view this change? | push the stomach anteriorly
|
Following pancreatitis (inflammation of the pancreas), the posterior wall of the stomach may adhere to …? Why does this occur? |
|
Hiatal Hernia |
(often distressful and cause pain) |
What are 2 main types of hiatal hernias? Which people are these most likely to occur in? | paraesophageal hiatal hernia + sliding hiatal hernia
(possibly b/c of weakening of muscular part of diaphragm + widening of esophageal hiatus) |
Paraesophageal hiatal hernia |
(cardial orifice is in its normal position)
|
Sliding hiatal hernia |
= some regurgitation of stomach contents into esophagus |
Congenital Diaphragmatic Hernia | part of the stomach + intestine herniate through a large posterolateral defect in diaphragm (foramen of Bochdalek)
|
Congenital Diaphragmatic Hernia: With abdominal viscera in the limited space of the prenatal pulmonary cavity, the lungs (especially the left lung) does not have room to develop. What is the mortality rate in these cases? | high = approximately 76% (b/c of consequent pulmonary hypoplasia) |
The stomach has a rich arterial supply arising from ____________? | the celiac trunk and its branches |
Most blood is supplied to the stomach by anastomoses formed - |
|
The gastric veins parallel the arteries in position and course. The right and left gastric veins drain into what vein? | the portal vein |
The short gastric veins + left gastro-omental veins drain into the _____________? | splenic vein |
The right gastro-omental vein empties in the __________? | superior mesenteric vein |
Which 2 veins join to form the portal vein? | splenic vein + superior mesenteric vein |
What vein is used by surgeons for identifying the pylorus? Where is it located? | prepyloric vein (because this vein is obvious in living persons)
|
The gastric lymphatic vessels accompany the arteries along the greater and lesser curvatures of the stomach. They drain lymph from which surfaces toward its curvatures? Which lymph nodes are located here? |
|
gastric lymph nodes drain from what area of the stomach? | superior 2/3 of the stomach (along the right and left gastric vessels) |
pancreatico-splenic lymph nodes drain from what areas of the stomach? | fundus + superior part of the body of the stomach (drains along the short gastric arteries and left gastro-omental vessels) |
Lymph from the right 2/3 of inferior third of the stomach drains along the right gastro-omental vessels to which lymph nodes? | pyloric lymph nodes |
Lymph from the left 1/3 of greater curvature drains along the short gastric + splenic vessels to what lymph nodes? | pancreaticoduodenal lymph nodes |
The parasympathetic nerve supply of the stomach is from the vagal trunks and their branches? where do they enter the abdomen? | anterior and posterior
|
The anterior vagal trunk (mainly from left vagus nerve - CN X), lies on the anterior surface of the esophagus. It runs toward which area of the stomach? | lesser curvature |
The larger posterior vagal trunk (mainly from right vagus nerve), enters the abdomen on the posterior surface of the esophagus. As it passes toward the lesser curvature of the stomach, what does it gives off? | a celiac branch | (runs to the celiac plexus) |
The sympathetic nerve supply of the stomach comes from which spinal nerves? | T6 - T9 segments of the spinal cord |
The sympathetic nerves of the stomach pass to the celiac plexus through the which nerve? Which plexuses are they distributed through? | greater splanchnic nerve plexuses around the gastric + gastro-omental arteries |
Pylorospasm | Spasmodic contraction of the pylorus sometimes occurs in infants (usually between 2 and 12 weeks of age)
|
Congenital Hypertrophic Pyloric Stenosis | thickening of the smooth muscle in the pylorus (approx. 1 in 150 male infants; 1 in 750 female infants)
|
Carcinoma of the Stomach |
|
gastroscopy | can inspect mucosa of the air-inflated stomach
|
In the case of stomach carcinoma, the lymp nodes along the splenic vessels can be excised by removing what structures? | spleen gastrosplenic + splenorenal ligaments body + tail of pancreas |
Carcinoma-involved nodes along the gastro-omental vessels can be removed by resecting the greater omentum. The removal of the which lymph nodes prooves more difficult? | aortic nodes celiac nodes nodes around head of pancreas |
Gastrectomy (Total gastrectomy vs. Partial gastrectomy) | Total = removal of the entire stomach (uncommon) Partial = removal of part of the stomach ( ex. region of the stomach involved by a carcinoma) usually also requires removal of all involved regional lymph nodes |
Arterial anastomoses supplying the stomach are clinically beneficial during gastrectomies because…? | one or more arteries may be ligated during procedure (without seriously affecting blood suppling remaining stomach) |
Cancer frequently occurs in the what region of the stomach? It is important to remove which lymp nodes in these cases? | pyloric region Important to remove:
(receiving lymph drainage from this region) |
As stomach cancer advances, lymphogenous dissemination of malignant cells involves which important lymph nodes? | celiac lymph nodes | (all gastric nodes drain here) |
Gastric Ulcers |
(peptic ulcers = lesions of pyloric canal or duodenum mucosa)
|
Individuals with gaastric ulcers often have gastric acid secretion rates that are _ times higher than normal between meals. | as much as 15 times higher *thought that high acid in stomach/duodenum overwhelms the bicarbonate normally produced by duodenum ---> reduces effectiveness of mucous lining = vulnerable to H. pylori* |
How does the Helicobacter pylori (H. pylori) effect the stomach, causing ulcers? What can happen if ulcers erode into gastric arteries? | bacteria erodes protective mucous lining of stomach = inflamed mucosa; vulnerable to effects of gastric acid + digestive enzymes (pepsin) produced by the stomach if gastric arteries erode = can cause life-threatening bleeding |
secretion of acid by parietal cells of the stomach is largely controlled by the vagus nerves. What procedure is performed in some people with chronic or recurring ulcers to reduce the production of acid? | Vagotomy (surgical section of the vagus nerves) may also be in conjunction with resection of the ulcerated area |
truncal vagotomy | (surgical section of the vagal trunks)
|
selective gastric vagotomy |
|
selective proximal vagotomy |
|
A posterior gastric ulcer may erode through what structures? This results in …? |
|
In a posterior gastric ulcer, erosion of the splenic artery results in what? | severe hemorrhage into the peritoneal cavity |
Pain impulses from the stomach are carried by what type of fibers that accompany sympathetic nerves? | visceral afferent fibers The pain of a recurrent peptic ulcer may persist after complete vagotomy, whereas patients who have had a bilateral sympathectomy may have a perforated peptic ulcer and experience no pain |
Visceral Referred Pain: Why is pain from a gastric ulcer referred to the epigastric region? |
(supplied by the same sensory ganglia and spinal cord segments) |
The surface markings of the stomach in the supine position include: | Cardial orifice = posterior to 6th left costal cartilage, 2 - 4 cm from the median plane at the level of the T11 vertebra Fundus = posterior to left 6th rib in plane of the mid clavicular line Greater curvature = passes inferiorly to left as far as 10th left cartilage before turning medially to reach pyloric antrum Lesser curvature = passes from right side of cardia to pyloric antrum; most inferior part of curvature marked by angular incisure (lies just left of midline) pyloric part of stomach * |
Where are the surface marking for the pyloric part of the stomach in the supine position + the erect position? | supine position = level of the 9th costal cartilages + level of L1 vertebra; pyloric orifice is approximately 1.25 cm left of midline erect position = right side; location varies from L2 through L4 vertebra |